
I am featured in the recent AARP magazine! Read on…
https://www.aarp.org/health/conditions-treatments/info-2018/medical-experts-insider-advice.html
I am featured in the recent AARP magazine! Read on…
https://www.aarp.org/health/conditions-treatments/info-2018/medical-experts-insider-advice.html
Why are you hoarse? What should you do? There are a multitude of causes of hoarseness. Hoarseness is a common presentation to primary care physicians. The causes range from inflammatory processes to psychiatric disorders to more serious systemic, neurologic or cancerous reasons.
Medication can also cause hoarseness. The medications that may cause hoarseness are angiotensin-converting enzyme inhibitors (ACE) , antihistamines, diuretics, bisphosphonates, and inhaled corticosteroids.
How to evaluate hoarseness? Your physician should perform a targeted history and physical exam. Systemic conditions causing hoarseness should also be investigated. Initial treatment may be voices rest including no whispering (as this can worsen hoarseness) and treatment of the presumptive cause.
If you have reflux, the acid from the stomach can affect the vocal cords and cause hoarseness or a chronic cough from acid reflux (or lung cancer) can also cause hoarseness. Direct visualization with a nasolaryngoscope (a teeny tiny scope about 1/2 the size of your pinky finger) may be needed if hoarseness persists for 3 months if conservative management has not resolved the problem. An ear, nose, throat surgeon may do this in their office. If you have risk factors for oral cancer like tobacco use or heavy alcohol consumption or blood with coughing should opt for ENT referral after 2 weeks of symptoms.
Don’t I need imaging? Probably not. A CT scan is not done before visually examining the area with a nasolaryngoscope.
Voice therapy is effective for improving voice quality for patients with nonorganic difficulty with making sounds.
When do you need surgery? Surgery is needed for laryngeal or vocal fold dysplasia (or cancer!), airway obstruction, or benign pathology that is resistant to conservative treatment. 
The USPSTF (United States Preventive Services Task Force) is a conservative group that reviews data to give guidelines for physicians. The USPSTF has recently given recommendations on WHO should be screened for sleep apnea.
Who should NOT be screened for sleep apnea?
What are symptoms of obstructive sleep apnea?
How can treatment of obstructive sleep apnea help patients?
Does using CPAP decrease mortality or cardiovascular events (like heart attack and stroke)?
 No. The USPSTF did not find that CPAP decreases these outcomes.
No. The USPSTF did not find that CPAP decreases these outcomes.
Radon. What is it? Should I test for it? Should I even be concerned?
Radon is a unique environmental health risk. It comes from uranium and radium natural decay. Radon is a greater source of natural radiation than exposure to the sun, x rays or other medical devices.
Is this important? Yes. The Environmental Protection Agency (EPA) estimates that radon causes approximately 100,000 lung cancer deaths in the US yearly. Radon is considered the seventh-leading cause of cancer-associated death in the US.
How to measure radon? Measure radon with a home kit. Kits cost $15-25 and you use them in the home for 2-7 days. If a home has a crawl space, test the living area above the crawl space. Radon is measured in picocuries per liter of air (pCi/L). If you smoke 8 cigarettes/day that equals 4.0 pCi/L. Do not measure the soil level of radon.
What level is significant? 4.0 pCi/L is the level at which radon mitigation should be initiated.
How to mitigate radon? Active or fan-powered soil depressurization is a standard approach to radon reduction and mitigation. This may typically cost $1500. Each state has different certification and license requirements to be a radon mitigation service.
Do you need to retest? Yes, if the home has “settled” or the foundation has had structural changes.
How many homes have elevated radon levels? 6% of all US homes have radon levels over 4.0 Ci/L. But, different parts of the country can vary greatly. (70% of Iowa homes have elevated radon levels).
Want more information? Call the National Radon Program Services (with the EPA) at 1-800-557-2366. They are also known to have radon kits! or radon kit coupons.
I hope this helps.
Nevada has instituted a new controlled substance law for prescribers to follow…. or else!
I recently attended a 2-hour evening session informing me of the details of the new Nevada AB474, Nevada’s opioid prescribing law. Unless your head has been in the sand, you must know that there is an opioid crisis. Nevada’s government has decided that to decrease the abuse, they should make the prescribing cumbersome and onerous. I have had patients ask me for a benzodiazepine to take before a flight. This now requires an online data search of the patient’s PMP, risk factors, alternatives, evaluation, and a signed informed consent form. I took notes at my meeting and have included them below…
AB474. This is the Nevada law that was enacted January 1, 2018 and it has turned controlled substance prescribing on its head.
Here are the following requirements…
Controlled prescriptions needs to have four components written on the prescription.
As a physician, we are required to have 2 hours of continuing medical education per year specifically about opioid prescribing. This evening met that requirement for this year. Hooray!
The office note needs to document the following.
“Informed consent” form needs to be obtained from the patient. The informed consent must contain
How many days of medication can be prescribed for the first prescription? 14 day maximum for pain relief. Some pharmacies only fill 7 days worth of pain medicine (this is the rule of those specific pharmacies).
Risk factors. There are 16 risk factors to review with each patient before a prescription is written.
Prescription Medication Agreement (must be completed on all patients on controlled substances for more than 30 days) include
The patient must perform a urine drug screen, if the physician asks for it.
The patient needs to inform the physician if they use any other drugs (including marijuana) and if they are having any side effects.
At 90 days, an evidence-based work up of the medical condition has been initiated. For instance, if the pain medicine is being used for back pain, has the back pain been worked up appropriately? Have non-controlled substances be tried and failed?
It the patient is taking more than 90 MME (morphine equivalents)? if so consider sending them to pain management physician as this falls outside the normal dosage range.
“Prescribe 365” This refers to the patients only receiving one years supply of rx in one year to help decrease duplicative rx. Or doctor shopping.
Long-term management of patients with controlled substance prescriptions.
Must be seen every 3 months for long-term pain management. Three prescriptions, each for one month, can be given to the patient at one visit (as long as the physician feels comfortable doing this.)
Controlled substance agreement needs to be signed by the patient once a year.
Resources www.nvdoctors.org or www.prescribe365nv.gov or http://bop.nv.gov/links/PMP/ or https://knowyourpainmeds.com is geared toward patients.
This is a powerful read. Assault weapons are a medical problem. Read on to appreciate the “smashed melon…”

Are you a woman concerned about breast cancer? There is a fantastic online tool to help you figure out your risk of having breast cancer.
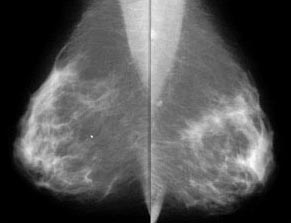
http://www.vhct.org breast cancer
https://www.cancer.gov/bcrisktool/
What kind of doctor is your “doctor?” I recently talked to a girlfriend who saw a practitioner but did not know their schooling or specialty.
You should care about and KNOW what kind of medical professional you are seeing. Do you? Here is a great article to help you know more about WHO you see and what their skill set is.
 Get involved in your care.
Get involved in your care.
Peanut allergies in infants. The New England Journal of Medicine published an update on peanut allergies in infants and what to do to decrease them.
Did you know?
A unique study, called the Learning Early about Peanut Allergy (LEAP) was conducted in children from 4 to 11 months with severe eczema, egg allergy or both. The study lasted until age 5. The prevalence of peanut allergy was 17.2% in those who AVOIDED peanuts and 3.2% among those who CONSUMED peanuts.
This study helped shape the guidelines that the National Institute of Allergy and Infectious Diseases (NIAID) made in 2017 that infants with severe eczema, egg allergy or both should consider peanut-specific immunoglobulin E measurement and/or skin prick test. Then, based on the test result, introduce age-appropriate peanut-containing foods as early as 4 to 6 months to REDUCE peanut allergy risk. For infants with no eczema or food allergies, they may have peanut-containing foods introduced at any age in accordance with “family and cultural preferences.”
I hope this helps.
Insurance company Medical director admits that denials made without looking at the chart?!
Interesting. And upsetting. If you, as a patient, have been denied imaging, testing, specialty referral…. there’s a chance it’s been denied without your case ever being reviewed.
Read on….
https://www.cnn.com/2018/02/11/health/aetna-california-investigation/index.html

You must be logged in to post a comment.